How to improve value-based care with contract lifecycle management
07/12/2024
11 min read

Value-based care aims to improve healthcare outcomes while reducing costs. Despite its potential, the rollout has been slow and inconsistent. At a recent Healthcare General Counsel Conference, only one out of 30 participants indicated they were involved in value-based contracts. However, a 2022 study found 76% of healthcare organizations had commercial value-based contracts, and 74% had Medicare Advantage value-based contracts. This discrepancy highlights the challenges in implementing value-based care.
Challenges in Value-Based Contracts
Thomas Cowen, Head of Vertical Strategy - Healthcare & Life Sciences at Conga, identifies a key challenge: "Even when I ask different people in the industry for examples of the value of a contract, they often don't have any to give us. Standardization is one of the major challenges there."
Importance of Automated CLM Solutions
Automation becomes more critical in the transition from fee-for-service to value-based care for four reasons:
Complexity: In fee-for-service schedules, the complexity resides in long fee schedules with hundreds or thousands of procedure-based CPT fees. Despite the volume of data that must be derived and placed in the contracts, it is a laborious but straightforward task. Simply determine the range of procedure codes and then the rates.
Value-based grids, on the other hand, are smaller in size and calculation. The complexity lies in the definition during the program inception, and the metrics represented on the contract and defined in a table—albeit not thousands of lines long. The data processing involves intimate knowledge and reference to the definitions, the meaning, and the pitfalls of every word.
Tom Cowen explains, "The marriage of structured data from contracts with unstructured data at the fee schedule level is a beautiful one. It allows you to readily access your contracts and fee schedule addendums and match that to your claims system to see if it's actually benefiting both parties."
Intention: This is the more interesting and perplexing difference between the two types of arrangements. As mentioned, the tasks on fee-for-service contracts are straightforward. That is because the intent of the contract is clear and has been for decades. Physicians and providers provide services and payers pay for them. A defined coding structure yields a predictable result.
Value-based contracts require that both parties come to terms, whether stated explicitly or implicitly. The definition of that intent, alignment of the intent to representative metrics, and definition of language that captures the intent are all paramount to a successful contract and, more importantly, a sustainable relationship.
Data collection, integration, and interoperability: As mentioned above, value-based contracts require new metrics, which means new data. Value-based data must be collected, integrated, and interoperable between systems—from the CLM to back-end systems. This data comes from patient test results contained in an electronic health record (EHR), meaning new tables or modules of the EHR may need to be collected. Multiple data points from different systems may need to be integrated. Value-based care tests the backbone of data from the payer to the provider as never before. This test is not a one-time data retrieval but must be automated, allowing different payers to work with different providers.
Changing policies and programs: The nature of government is constant change. With every new election, changes in legislature bring change in Medicare program approach and funding. This change is often glacially slow, but when it happens, the shifts can be sweeping in nature. Systems and processes that support value-based care must be agile and flexible to these changes, built on a solid footing.
Tammy Hawes, CEO and Founder of Virsys12, emphasizes that implementing new business models in healthcare to enhance quality and reduce costs for member populations requires robust automation and structured systems. She warns that without advanced technology, the administrative demands of these new organizations could diminish or even nullify the overall savings achieved.
Crafting Effective Value-Based Contracts: Key Principles and Practices
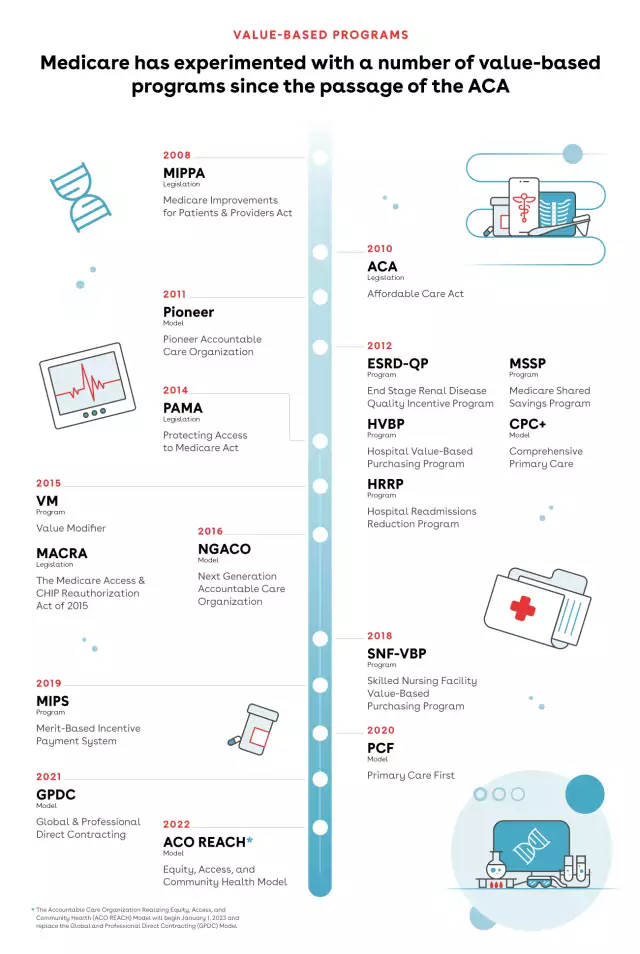
Value-based contracts take different forms based on their program. Performance-based programs are different from shared savings models. Capitated programs will differ from bundled payment models. You can see the evolution of value-based legislation and contracts here:
Effective value-based contracts are clear and unambiguous in their language and intent. Contract language and metrics should adhere to the following principles:
- Focus on value: The contract should clearly define how value is measured: by savings, patient counts, or performance. These can include quality of care, patient outcomes, and cost-effectiveness metrics.
- Mutual understanding: Both parties (provider and payer) need to be on the same page regarding the program's intent and its ultimate effects on the patient population.
- Transparency: The contract should be transparent throughout, particularly around how payments are determined and what actions qualify for incentives or penalties.
While legal language might be necessary for particular clauses, the core of the contract should be easy for everyone involved to understand. Payers and providers have different perspectives that must be clear to both sides.
At a more detailed level, we recommend that you focus on the following:
- Specific definitions: Clearly define critical terms like quality measure, patient outcome, and cost effectiveness. Clear language avoids ambiguity and potential disputes down the road.
- Performance metrics: Outline the specific metrics used to assess performance and how data will be collected and reported.
- Dispute resolution: Establish a process for resolving any conflicts that may arise during the contract term.
Work to leverage your CLM solution to automate this process. For example:
- Instantiate clauses negotiated well with both sides' perspectives, making those the default clauses for the various program types.
- Dynamically populate contract templates with those clauses based on the program framework variables contained in the contract request form.
- Establish pre-approved fallback language that business users can substitute.
The goal is a clear and understandable document that fosters a successful value-based care arrangement. Create a process to continually refine contract language and definitions moving forward as disputes and issues arise. Language that seemed clear when the contract was authored may not be adequate once the contract is implemented. Care and feeding of your value-based contract lifecycle will deliver better results for your organization and, most importantly, your patients.
Combining Structured and Unstructured Data
Contract data structures vary between the many types of value-based programs dating back to the Centers for Medicare & Medicaid Services (CMS) original programs:
- End-Stage Renal Disease Quality Incentive Program (ESRD QIP)
- Hospital Value-Based Purchasing (VBP) Program
- Hospital Readmission Reduction Program (HRRP)
- Value Modifier (VM) Program (aka Physician Value-Based Modifier or PVBM)
- Hospital Acquired Conditions (HAC) Reduction Program
From our experience, most value-based contracts currently contain unstructured data that is hard to find and leverage in future agreements. The key is to focus on an implementation that supports a move to structured data. Contract lifecycle management brings structure to this unstructured environment in many ways that we'll outline below.
CLMs drive process automation through automated approval requests, dynamically generated drafts, and pre-approved clauses. Users gain intelligence via a holistic view of in-flight and activated value-based contracts, insight into clause modification hotspot areas, and easy access for authorized users. An effective CLM system turns unstructured data into structured data in the following ways:
Legacy import: AI-based legacy contract ingestion creates metadata from large language model-based data interrogation. Key fields like start and end dates, party names, and payment terms are easily identified, while clauses specifying contractual intent specified by your CLM provider are more challenging. Once identified, clauses and metadata are easily searched for and reported on within your system.
We recommend having the AI identify your most used and important clauses and metadata. Import not only your value-based contracts but also your fee-based schedules, as they will inform your clause library and provide valuable information in future negotiations.
Third-party paper: Depending on which side of the value-based contract your institution is on, you may or may not need to deal with third-party paper. Our experience shows that the payer authors most value-based contracts. Providers can benefit from utilizing the AI-based ingestion mentioned above for single third-party paper reads.
Clause library: Clause libraries enforce structure in your contracts with automated clause generation and identification. If you haven't already created a clause library, we recommend doing so. Leverage the findings of your legacy ingestion to identify your favored clauses and formalize them in your clause library.
Templates: Think of your template library as an extension of your clause library, adding key metadata fields captured in your agreement record. Locking key fields and sections of your templates from third-party edits will help to establish the line and keep control of your structured data.
Smart fields and clauses: Mark most of your fields and clauses as smart. This assists in automating changes from your Word documents to the agreement record. This two-way sync ensures that data is always accurate and available for reporting, approval processes, and search.
Tammy Hawes highlights, "Having contract data in a structured format also enables seamless integration with downstream systems, such as claims systems for provider payment activation, and other internal systems used for provider and practitioner communication."
Future-proofing and closing the loop
Strong discipline and processes will lead to a flexible, scalable CLM system that supports value-based contracts. Expect that legislation will change and that various parties will be unhappy with their programs. Be willing to change to strike balanced agreements that stand the test of time. Design for changing data standards and system upgrades. To do so, we recommend the following:
Listen to your business users: Business users are closest to the problems that will inevitably arise from a new way of doing business. Establish plans for regular communication with your business teams (account executives, finance, payables/receivables). When is business getting blocked or payments disputed? Identify the root cause of the dispute and take action on the very next contract you negotiate. Update the clause in your clause library with the new, improved language.
Prioritize reporting: Reporting should be a key foundation to a sustainable system. Set up reporting for all levels of the organization that focuses on the key metrics you have defined. Metrics reporting drives value-based care. This is important to both make payments and deliver care. Still, it is essential to manage the contracting process, ensuring that your operation can scale and identify issues ahead of time. Are you able to answer questions such as:
- Is a standard clause getting negotiated on every contract?
- Is there a business group that is slowing the cycle time?
- Are there contracts that should be automated (e.g., NDAs) but aren’t?
Formalize approval policies: Report on your approvals and continually tune your approval levels, adding new approval policies where needed. We recommend looking at the approval acceptances. If an approval is granted 95% of the time or more, it probably doesn't have any basis—or maybe your approvers are receiving too many approval requests. Did you discover a major dispute that arose from a certain clause or metric? Flag that item for VP or C-level approval in the future.
Follow the trends: Read the news and speak with team members who have intimate knowledge of impending legislation or trends. Talk with your account teams to understand how the other parties respond to their current contracts. How will their experience impact the next negotiation? How might they affect your existing and in-flight value-based contracts?
In addition to the recommendations above, Hawes emphasizes the importance of change management and how crucial it is for implementing any new technology. Contract management solutions, which impact various departments and systems within a business, require tightly aligned business units and strong collaboration to ensure successful implementation.
Managing your value-based contracts should be approached much like your other systems. But act with hyper-vigilance, as value-based contracts are vital to your business and change dramatically during implementation. In particular, look to deliver value, mutual understanding, and transparency in your contracts by focusing on definitions, metrics, and dispute resolution.
Place a strong emphasis on creating a structured data repository utilizing modern contract lifecycle software and discipline. The AI capabilities are compelling, but don't forget to focus on process, scaled delivery, and effective use of clauses and templates. Finally, focus on qualitative components by speaking with your experts and field users to understand trends and impending legislation that may change the delivery of value-based contracts.
About the authors:
Tom Cowen is a software industry veteran with over 30 years of experience in Sales, Contract and Price Management. Tom has spent the previous nine years at Conga and is the Head of Conga’s Healthcare & Life Sciences practice, reporting to Conga’s Chief Product Officer. His customers include leaders in the Pharma, PBM, Payer and Med Device spaces and work focuses on key HLS industry use cases. Prior to that, Tom was Director of Product Strategy at Vendavo, a leader in the Price Optimization space. Tom spent 15 years as a Global and Enterprise Sales Manager at market leading technology companies: Oracle, EMC and BEA Systems. As a Global Sales Executive, Tom managed, firsthand, the Sales and Negotiation Process as a supplier to top Pharmaceutical Manufacturers in the New York region.
Tom holds an MBA in Finance and BS in Marketing from New York University’s Stern School of Business and an MFA in Creative Writing from Salve Regina. He is the founder of Justin's Smile Childhood Cancer Foundation which funds pediatric cancer research and patient and family programs.
Tammy Hawes is CEO and Founder of Virsys12, a leading provider of SAAS products that empower healthcare organizations to eliminate inefficiencies in provider data management and workflow processes. Hawes launched Virsys12 in 2011, with a track record of more than 25 years of executive success. Prior to establishing Virsys12, Hawes’s held executive technology positions at Primex, Paradigm Health, Theraphysics and Behavioral Healthcare and served in CIO and CTO roles in these organizations after her early career as a software engineer. The Mississippi native received a BS degree in Computer Science from East Tennessee State University.
-
Only the Agile Thrive BlogIndustry InsightsOnly the Agile Thrive
Discover how business agility, AI, and connected data help companies respond faster to tariff disruptions, reduce risk, and make confident go‑to‑market decisions.02/23/20265 min read -
The contract management strategy you might be overlooking BlogCLMThe contract management strategy you might be overlooking
Discover the contract management strategy that improves collaboration, clarity, and results—without overcomplicating your process.07/15/20255 min read -
Ultimate guide to contract management GuidesCLMUltimate guide to contract management
Learn more about how effective contract management can help you streamline processes, maximize deal values, and reduce risk.
10/10/20200 min read -
Conga Recognized as a Leader in Five G2 Grid® Reports BlogCLMConga Recognized as a Leader in Five G2 Grid® Reports
Conga earns G2 Leader recognition for Contract Lifecycle Management and Document Generation, including #1 rankings for Enterprise Usability and Enterprise Relationships, based on verified customer reviews.01/22/20264 min read



